
Finally, 4+ years after the Covid Pandemic began, the General Public can finally see that Public Health Officials told us BOLD FACED LIES about the Covid vaccines' Safety and Efficacy. And I'm furious about it. I've had friends pass away during the pandemic after vaccination, and many are still experiencing serious health issues.
I tried to warn all my friends and family about the dangers of the vaccines, but they found it so hard to believe our government officials and the mainstream media would withhold this important data from us, many of them chose to get vaccinated anyway.
Please have a look at the videos on this page, so you can see what the Mainstream Media and Goverment Officials refused to disclose to the general public.
You may also want to read these posts:
- How The Mainstream Media Manipulates What We Believe About The Pandemic
- How Big Pharma Controls The Mainstream Media
- The C.D.C.: What You Need to Know (They Profit from Vaccines!)
- The F.D.A.: What You NEED TO KNOW (They KNEW The HIGH RISK of Potential DEADLY Vaccine Side Effects)
- In Fauci We BUST - Endless Evidence that shows why we can NO LONGER TRUST Tony Fauci
TOP VACCINOLOGISTS FAIL TO PRODUCE SCIENCE TO SUPPORT SAFETY
You MUST understand what A.D.E. (Antibody Dependent Enhancement) is, before you make an Informed decision about whether you want to get vaccinated (or get a Booster Shot)
What is Antibody-Dependent Enhancement?
From THIS PAGE:
"The simple definition of ADE is 'raising antibodies that don't protect, but actually make a viral infection even worse'. And obviously, that's the opposite of what you want." -Tony Fauci
Yes, Tony Fauci actually admitted this could happen.... and that is exactly what is happening right now. You can see lots of videos on THIS PAGE, that show how the unvaccinated are catching Covid at a greater rate than the unvaccinated are. You can see Fauci admit the vaccine could make people worse, in the video below (he just doesn't address the problem by it's name, A.D.E., but he uses the word "enhancement").
Fauci literally says, in this video: "It's the worst possible thing you can do."
FAUCI ADMITS: VACCINE CAN MAKE YOU WORSE!
Fauci knew this could happen. He is the highest-paid official in our entire government, with an extensive history of corruption. He knew exactly what was going on. The FDA even issued a report that showed all the serious side effects that could happen (like Guillan-Barre syndrome), before the vaccines were released. You can see their slide presentation in the first video on THIS PAGE.
Giving a vaccine that could cause ADE might not seem like such a crime if there were NO other treatments available, but given the fact that Fauci went out of his way to cover up the safety and effectiveness of Hydroxychloroquine, Ivermectin, Budesonide, and Monoclonal Antibodies, in favor of drugs that would make him and his buddies BILLIONS in combined profits.... there is no excuse. This tyrant needs to be held accountable.
One of the most frightening aspects of A.D.E. is that it can cause auto-immune conditions and a disease that's being coined as VAIDS (Vaccine-induced Auto Immune Deficiency Syndrome).
You can learn all about A.D.E. in the videos below.
(THE DANGEROUS) 'ANTIBODY-DEPENDENT ENHANCEMENT' PROBLEM WITH ALL CORONAVIRUS 'VACCINES'
ARE WE STARTING TO SEE A.D.E.?
Boosters May Weaken The Immune System Says European Medicine Agency (EMA) | T Cell Exhaustion
A MUST-READ....
Robert F. Kennedy Jr. and Del Bigtree explain A.D.E. in the video below, but here is a transcript of what they said.
RFK Jr:
“The government’s been trying for almost 30 years to develop a coronavirus vaccine and it’s been unsuccessful. And, beginning in 2002, there were 3 outbreaks of coronavirus, we called them SARS at that point, and MERS, and the first SARS was a natural illness that jumped from a bat to human beings. The second two were lab-created and had escaped and infected human beings.
And so the governments of China and a consortium of western governments all got together and put millions and millions of dollars into an effort to develop a coronavirus vaccine. And between 2002 and 2012, 2014 they worked very hard to do that.
And what happened is, they developed about 35 vaccines, and 4 of them were really promising. They chose the 4 most promising, and they gave them to ferrets, which is the animal that is most analogous to human beings when it comes to upper lung / respiratory infections. The ferrets had a brilliant, robust and durable antibody response. But then, something horrible happened. When those ferrets were challenged, when they were exposed to the wild virus, they got horribly sick. They got inflammation throughout their bodies, and they died.
And the scientists remembered that something very similar had happened in the 1960s where there was, where they had developed a vaccine for RSV, which is very similar to coronavirus, it’s an upper respiratory infection ailment. They had skipped the animals and given them directly to 35 children, and the children, again, had developed a very robust antibody response. But when those children were exposed to the wild virus, they got very very sick, much sicker than unvaccinated children, and two of those kids had died. It was a scandal.
And they realized, when the same thing happened with the ferrets, that there was something that they called “enhanced immune response.” It’s also called pathogenic priming. And what it means, is that when you get the vaccine, it appears that you have an antibody response, but when you actually encounter the wild virus, you become much sicker, and it actually creates a pathway that that virus hurts you a lot more than with unvaccinated people.
So this was 2012. In 2014, the NIH, under Fauci, developed a dengue vaccine, which had some signals in it that there was pathogenic priming. In other words, in the clinical trials, they saw some signs that you could get an antibody response but get much sicker, when you were exposed, but they ignored them. They gave it to the Phillippines, and they gave hundreds of thousands of children this vaccine, and when the dengue came around, those children became horribly ill, and 600 of them died. In the Philippines today, people are being criminally prosecuted for that.
So, the danger of the coronavirus vaccine is, you really need to test them on animals first, to make sure whatever the vaccine is, that we don’t get that really great immune response, followed by lethal infections. And it’s very very strange to me, and it almost seems criminally reckless, that Anthony Fauci is allowing these companies to skip animal trials and go directly to human trials."
Del Bigtree:
"I think if you think about it, too, what he’s talking about, how dangerous that is. Every scientist involved with this will say we don’t know why these antibody immune enhancement reactions happen. They don’t know why it happens. So, imagine that you have 100 companies right now, in this amazing race to make a vaccine, that could literally make them about 750 billion dollars, if they win it. But what happens if they’re testing it on a virus, right, they're going after a specific virus, but now we have 30 mutations already, of coronavirus, some of them very significant changes in the protein.
What happens if you made a vaccine that actually gets over this problem, that they know is a problem, that Tony Fauci is saying publicly, there’s a chance that this could make people more sick, so that we have to be very careful. What happens if they think they got around it, right, and they put out the vaccine. Bill Gates gets his wish, and Tony Fauci, everyone’s forced to take it around the world. Then all of a sudden, a mutation comes around, and we start seeing it trigger this antibody immune enhancement in people that are vaccinated.
Only problem now, if we’ve all got this vaccine, and now we’re not having a .1 to .3 percent death rate, it’s 20% or 30%, people are having the same issue as the ferrets. You could honestly wipe out our species with a vaccine that was rushed to market, that didn’t do proper safety testing. And that’s exactly what they’re describing this as. They’re putting 2 of the most dangerous words together, in every article, about this vaccine. Rushing, and Science. Those 2 words should never be in a sentence together!
ROBERT F. KENNEDY JR. EXPLAINS ADE (ANTIBODY-DEPENDENT ENHANCEMENT)
In the video below, Dr. Ryan Cole says:
"...What we're seeing in the laboratory after people get these shots, we're seeing a very concerning, locked in low profile, of these important killer T cells that you WANT in your body. It's almost a reverse HIV.
In HIV you'll lose your helper T cells, your CD4 cells. In this virus post-vaccine, what we're seeing is a drop in your killer cells, your CD8 cells. And what do CD8 cells do? They keep all other viruses in check.
What am I seeing in a laboratory? I'm seeing an uptick of herpes family viruses, I'm seeing herpes, I'm seeing shingles, I'm seeing mono, I'm seeing a HUGE uptick in human papillomavirus, in the cervical biopsies and the cervical pap smears in women. In addition to that, there's a little infectious bump that kids get called molluscum contagiosum. What do you need, to keep that in check? You need CD8 killer T cells. I'm seeing a 20x increase in individuals over the age of 50 of this little bump and rash. It's innocuous, but what it tells me is the immune status of these individuals who got the shot, were literally weakening the immune systems of these individuals.
Now, most concerning of all, is there's a pattern of these types of immune cells in the body that keep cancer in check. Well, since January 1 in the laboratory I've seen a 20x increase of endometrial cancers over what I see on an annual basis. A 20x increase. I'm not exaggerating at all. Cause I look at my numbers, year over year, I'm saying gosh I've never seen this many endometrial cancers before.
I'm seeing invasive melanomas in younger patients. Normally we catch those early and they're thin melanomas. I'm seeing thick melanomas skyrocketing in the last month or two. I'm already seeing the early signals. And we're modifying the immune system to a weakened state. A great study out of Germany that looked at these profiles on young individuals, after the Pfizer, showing this locked in, and we don't know how long, maybe the immune system's going to regenerate, and those ratios will go back up, but who's studying it? And where are the long term trials? Two months, 4 months? How long is this profile locked in? We don't know."
COVID “VACCINES” ARE LOCKING IN SUPPRESSED IMMUNITY, MAKING PEOPLE MORE PRONE TO HIV, HPV, SHINGLES
ADE in Severe COVID Causing Massive Inflammation and Immune Cell Death (Study Reveals)
Summary - ADE in Severe COVID Causing Massive Inflammation
CV ‘VACCINES’: THREAT SUMMARY OF “ANTIBODY-DEPENDENT ENHANCEMENT” (WORKING LINK IN DESCRIPTION)
5 Mechanisms of ADE (How Does Antibody Dependent Enhancement Occur?)
Cytokine Storm with ADE - Antibody-dependent Enhancement of Coronavirus
INTERVIEW WITH DR. DAN STOCK ON ANTIBODY DEPENDENT ENHANCEMENT, VITAMIN D
LUC MONTAGNIER - COVID JAB IS CAUSING ANTIBODY-DEPENDENT ENHANCEMENT AND CREATING NEW VARIANTS
ANTIBODY DEPENDENT ENHANCEMENT WORSENS OVER TIME [2021-10-04] - MIKE ADAMS (VIDEO)
DR. SUCHARIT BHAKDI: ANTIBODY DEPENDENT ENHANCEMENT IS A SERIOUS CONCERN FOR THE CV-19 VAXXED
BREAKING VACCINE DATA - ANTIBODY DEPENDENT ENHANCEMENT EXPLODING!
SITUATION UPDATE: CATASTROPHIC ANTIBODY DEPENDENT ENHANCEMENT INJURIES & DEATH - MIKE ADAMS (VIDEO)
NURSE EXPLAINS THE DELTA VARIANT IS ANTIBODY DEPENDENT ENHANCEMENT (ADE) FROM THE JABS
DR. ROBERT MALONE "WORST CASE SCENARIO” CITES FIRST EVIDENCE SHOWING ANTIBODY DEPENDENT ENHANCEMENT
STEW PETERS - DR. JANE RUBY BREAKING VACCINE DATA - ANTIBODY DEPENDENT ENHANCEMENT EXPLODING!
ANTIBODY DEPENDENT ENHANCEMENT AND AUTOIMMUNE DISEASE
COVID ANTIBODY DEPENDENT ENHANCEMENT - SPIKE PROTEIN LISTEN TO THIS DR EXPLAIN
(PART - 02) EMERGENCY SATURDAY 10/2/21 BROADCAST - DR RICHARD FLEMING ANTIBODY-DEPENDENT ENHANCEMENT
THERE WILL BE MORE DEATHS DUE TO ANTIBODY DEPENDENT ENHANCEMENT (ADE) CAUSED BY THE VACCINES
WHAT IS ANTIBODY-DEPENDENT ENHANCEMENT OR ADE?!?! PROF. DOLORES CAHILL
I learned about Dr. Leonard Horowitz for the first time after watching this video with Dr. Michael McDowell, who says Dr. Horowitz' findings have never been refuted. You can see an eye-opening video with Dr. Horowitz, below this one. Just be warned.... once you see it, you can't unsee it.
DR. MICHAEL MCDOWELL EXPLAINS VIRAL IMMUNE ESCAPE AND ANTIBODY DEPENDENT ENHANCEMENT (ADE)
DR. LEONARD HOROWITZ - A LECTURE ON EMERGING VIRUSES, HIV, POLIO, HEPATITIS, EBOLA
STEW PETERS - BREAKING VACCINE DATA – ANTIBODY DEPENDENT ENHANCEMENT EXPLODING! (9/15/21)
(ADE) R. KENNEDY JR. & DEL BIGTREE EXPLAIN ANTIBODY-DEPENDENT ENHANCEMENT (ADE) ON JONI
DR TENPENNY EXPLAINS THE DANGERS OF ADE - ANTIBODY DEPENDENT ENHANCEMENT FROM COVID VACCINES
DEL BIGTREE BREAKS DOWN HOW THE THE VAX HURTS YOUR IMMUNE SYSTEM
VACCINE EXPERT WARNS OF COVID VACCINATION CATASTROPHE
THEY ADMIT IT! - JAB IS THE VARIANT! - CAUSING DEATH & INJURY! - MASSIVE COVERUP EXPOSED!
COVID VACCINES "WIPE OUT" NATURAL ANTIBODIES
DR. CHETTY - WE HAVE SOME VERY, VERY TOUGH TIMES AHEAD - THE SPIKE PROTEIN IS INHIBITING CELL REPAIR
Dr. Paul Cottrell: The covid vaccine is a government bioweapons "antidote" gone awry
Please click on this link to read the article below, and consider subscribing to Jessica Rose's substack. She has some great posts!
https://jessicar.substack.com/p/the-bnt162b2-mrna-vaccine-against?s=r
'The BNT162b2 mRNA vaccine against SARS-CoV-2 reprograms both adaptive and innate immune responses'
It's all in the title...
 |
|

A brand new medRxiv pre-print study entitled: “The BNT162b2 mRNA vaccine against SARS-CoV-2 reprograms both adaptive and innate immune responses” has graced our world. This paper is so important and it provides evidence to support what many prominent immunologists and vaccinologists have been saying for a long time, including myself. These COVID-19 mRNA injectable products are causing, yes, causing, immune system dysregulation - and not just in the context of the adaptive system, but in the context of the innate system. Not only that, but these findings provide very good reasons as to why we are seeing resurgences of latent viral infections and other adverse events reported in VAERS (and other adverse event reporting systems) and perhaps more importantly, why we should under no circumstances inject this crap into our children. Children are fine in the context of COVID-19 (for the 80 millionth time - this well documented) and this is due to their extraordinary innate immune response systems.
Let’s rip into some background in immunology, shall we?
Figure 2 shows many of the different cell types involved in the adaptive and the innate immune system branches. Most of you probably know about T cells and B cells. I would bet that many more of you have not heard of my personal favorite killer, the Natural Killer (NK) cell. They kill infected cells and are of utmost importance to a healthy and functioning immune system. The cell types involved in the innate immune response system emit special molecules in response to invaders. These special molecules primarily comprise defensins, collectins, c-reactive proteins, lipopolysaccharide (endotoxin) binding proteins and complement factors. These responses are non-specific and target invading pathogens and even cancer cells.

In a nutshell, in this article, what they found was that the BNT162b2 (Pfizer/BioNTech) injectable products are modulating the production of inflammatory cytokines by innate immune cells upon stimulation with both specific (SARS-CoV-2) and non-specific (viral, fungal and bacterial) stimuli whereby the response of innate immune cells to TLR4 and TLR7/8 ligands was weaker after BNT162b2 injection, while fungi-induced cytokine responses were stronger.
In conclusion, the mRNA BNT162b2 vaccine induces complex functional reprogramming of innate immune responses, which should be considered in the development and use of this new class of vaccines.
Yes. It should be. And it should have been.
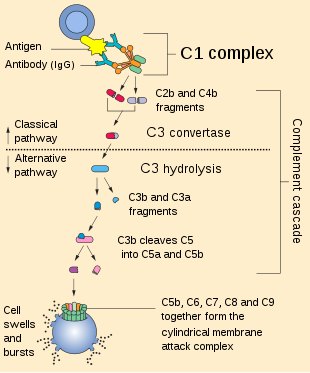
So what is inside the nutshell? Let’s back it up a bit, shall we? What are acquired/adaptive immune responses and more importantly, what are innate immune responses? I did say we were going to rip into immunology. Our immune system’s first line of defense is called the innate immune system. It comprises the skin (chock full of epidermal dendritic cells or Langerhans cells), mucous and mucosal epithelium, immune cells such as natural killer cells, basophils, dendritic cells, mast cells and macrophages and many molecular mediators such as cytokines, interleukins, c-reactive proteins and complement factors. The complement system (Figure 2) is an immutable system vital to proper functioning of antibodies and phagocytic cells (cells that eat stuff), clearance of invaders and damaged cells, inflammatory response promotion and membrane attack complex (MAC) formation (Figure 2). Membrane attack complex. Cool name for a band.
The mucus layer covering the mucosal epithelium acts as a first physical and biochemical barrier. An additional layer of physical protection against microorganisms is provided by a tightly interlaced cell-to-cell network of epithelial cells and intraepithelial lymphocytes. Various antimicrobial peptides produced by the epithelium and secreted into the mucosal lumen can directly kill the invading pathogenic bacteria.1
Every single ‘invader’ such as bacteria or viruses have molecules on their surfaces known as Pathogen-Associated Molecular Patterns (PAMPs) that are detectable by cognate molecules on immune cell surfaces call Pattern Recognition Receptors (PRRs). One type of PRR are Toll-like Receptors (TLRs). These TLRs come in many types and bind to specific types of molecules. TLR-7, for example, binds single-stranded RNA (ssRNA). Hmm. Where have I seen that before? Oh right! SARS-nCoV-2 is an ssRNA virus. Interesting. There are also cell receptors called RIG-I-like receptors (RLRs) that sense viral RNA.2
If a PAMP is detected by a PRR, an intracellular signalling cascade commences which results in the production of such inflammatory mediators as Nitric Oxide, histamine, TNF-alpha, IL-1 (protoypic inflammatory cytokine) and others as part of a pro-inflammatory reaction to quell invaders. Perhaps of primary note is that via TLR signalling - a prolific PRR type - Nuclear Factor kappa B (NF-kB) activation ensues. What is NF-kB?
NF-kB3 plays a key role in regulating the immune response to infection. Incorrect regulation of NF-kB has been linked to cancer, inflammatory and autoimmune diseases, septic shock, viral infection, and improper immune development.
In the presence of danger, the immune system responds via these fantastic on/off switches and mechanisms, to eliminate said dangers. This is the natural way of things and it is a constant ebb and flow of immune system regulatory magic.
Let’s assume the role of the coronavirus and see what our life would be like in the case of say, a child. You should know, once again, that children have very strong innate immune systems. The links attached refer to excellent works by Dr. Robert Malone and Dr. Francis Christian on this subject. So I’m a coronavirus and some arshole just sneezed me all over the face of a child standing next to me. The person who sneezed is one of those people who wears a mask incessantly on their chin and then sneezes all over everyone whilst symptomatic. So the child has me (Dr. Coronavirus or Dr. CV, for short) all over it’s face. And just so you know, there are many of me. So I find my way in a misty droplet into the sweet nasal cavity of this child where I encounter lots of mucousy membranes and sheets of epithelial cells. Lots of mucous. Mucosaliscious. I imagine it would be like running through a tunnel full of spider webs like Frodo Baggins did when he was trying to escape ‘she who needs to feed’ in order to get to the Mordor volcano to destroy the ring of power. So it’s kind of hard to get through. The nose. Sort of.
Ok, so most of me gets stuck in the booger path in the child’s nose. But nasal epithelial cells are chock full of ACE-2 receptors. I can bind them and thus can easily get inside the nice and warm cozy cells. There are also CD147 receptors here! So, a few of me manage to get ‘past’ this mucousy hurdle and bind to yummy epithelial cells via ACE-2 and CD147 receptors, which to me, are like red and yellow-colored lollipops of delight leading me into the place where I can call home and settle down and reproduce. But wait, before we get into that, since I am lurking around looking for receptors to bind, I am also encountering a lot of cells. These cells start telling me that they need to see my green pass if I want to keep lurking. No wait, no not my green pass, my PAMPs, so that they can find out how dangerous I am. I am new to this neck of the woods so they’re more than a little curious about my lurking. So they probe me with their PRR/TLR tools. Oh man! This is not pleasant at all! Being frisked by dendritic cells is like being manhandled by an octopus on a mission. So even though I have no idea, the by-product of their frisk is the inevitable launch of an army of things hell-bent on removing me from this kid. All of a sudden I’m surrounded by tenticular cells and they’re throwing TNF-alpha and IL-1 molotov cocktails at me! And it’s starting to get really hot in here and I’m like, man, this is not a hospitable environment. What did I do to deserve this? I’m just an innocent virus ultimately looking for a place to… breed.
Luckily, I have made a home in some cells. I am bound to others about to gain entry. But, the immune defenses don’t stop on the outside of cells; they continue on the inside. I thought I had found a nice warm and cuddly cell to settle down in and reproduce in. I have to think again! All of a sudden the PH is like, way too high! This feels awful! They’re trying to kill me, man! And eventually, they destroy me before I can get out. One of them sicked this crazy MAC on me and it poked holes in my home cell that I had managed to get into. They also used all sorts of internal and external armaments to make sure they cleared me out. And they did!
How do I know that? Because I am speaking from virus heaven.
So that’s the imaginary journey of the SARS-nCoV-2 virus and the potent response of a child’s innate immune system to my presence. Not enough cells get infected fast enough for an infection to ensue. The kid never gets to disease state and in most cases, symptoms are excessively mild or non-existent.
Alas, not enough of me were able to ‘infect’ enough cells to result in enough of me being produced to result in a ‘symptomatic infection’ party party. Innate immune system: 1. Coronavirus me: 0.
But what if I am reincarnated as mRNAs’ssss. And let’s go really sci-fi and imagine I am reincarnated as mRNAssss’s wrapped in a Lipid Nano Particle (LNP) bubble. And what if, I happened to be injected into someone’s arm muscle. What lives I am having! So what would be my fate? Well, surely, since I am injected intramuscularly with a pretty heavy guage needle (22–25-gauge 5/8 inch (16 mm)), I get inserted pretty deep and in copious amounts into muscle tissue. I witnessed many a muscle cell screaming in pain! I can’t really see anything yet because of this fat bubble I am in. But all of a sudden I feel us moving! So fast! The injector didn’t aspirate to check if I was being injected into the muscle as planned! It’s like riding the rapids of the cardiovascular system! Or something. Then suddenly we stop. There’s some kind of blurry kidney-shaped thing outside. It seems like the LNP has slimed its way into a cell. And I think we were just dumped out of the LNP into this cell. Well, ok. This is great news! Since we have been reincarnated into mRNAs, we can simply find ribosomes and start translating ourselves into the butterfly proteins we’ve always wanted to be! And there will be so much of us! Butterlies a swarmin’ in the body of a person! We have to act fast though, lest we be… degraded, however. I guess this is why we were wrapped in a LNP.
Later on that day…
So we are a spike proteins now! Hallelujah. We can do so many things! But we have to be careful: there are cells everywhere looking to eat us and turn us into alphabet soup. These so-called antigen-presenting cells just love to gobble up foreign proteins like us and regurgitate our entrails and mount them on Major Histocompatability Complex (MHC) I and II molecules. If they do that, then those T cells and B cells can detect our ground up guts mounted on these complexes and then build an army of cells that can recognize us and kill us! We do not want that. We want to exist. We seem to be doing alright in that desire. We also have to make sure that we don’t end up killing this person we got injected into! That wouldn’t help anyone, now would it. We can embed ourselves into monocytes4 and other cells like epithelial cells5 due to their proclivity to express ACE-26. But there’s a problem here. Through no fault of our own, we are causing some serious micro-clotting issues all over this person’s body by binding all these ACE-2 and CD147 receptors. The inflammatory mediators produced in response to our presence are in overdrive and the entire system is on fire! Hyperinflammation abound! The normal systems that regulate the anti-inflammatory response seem to be on vacation and it just won’t seem to stop. And it’s all because of little old me! Since I was designed to be pretty durable with my extra prolines and my pseudouridines, I am not easily get-riddable. [Word on the street says that my prolines aren’t preventing me from binding ACE-2 at all.] That would explain why so many of me are stuck in monocytes. Teehee. By the way, I forgot to mention, while I was inside the cell as mRNA, there were these TLR-7 molecules that seemed to find me very attractive. They detected some of me and in some cells, caused a chain reaction that obliterated us and the cell.7 TLR-7 is actually really important in the context of COVID-19 clearance.8
Perhaps the most successful part of our journeys, however, has been the avoidance of those pesky innate immune mediators in that kid’s nose. Phew, what a bullet we dodged there, right? So we got catapulted all over the body, triggered the T and B cells to respond accordingly with their specificness all along the way, but we avoided all of that other stuff. That’s some weird under-the-radar stuff right there.
Until this body flushes me out (which could take 15 months (see reference #4) unless they inject me again!) I am probably going to cause some systemic problems while I am here. Of these problems includes the dysregulation of the innate immune system, the (subsequent) induction of a hyper-inflamed environment and so many thrombotic events.
I think we can get into the paper now. This article was meant to be about the paper, not an immunology lesson. But it seems these things are simply not mutually exclusive.
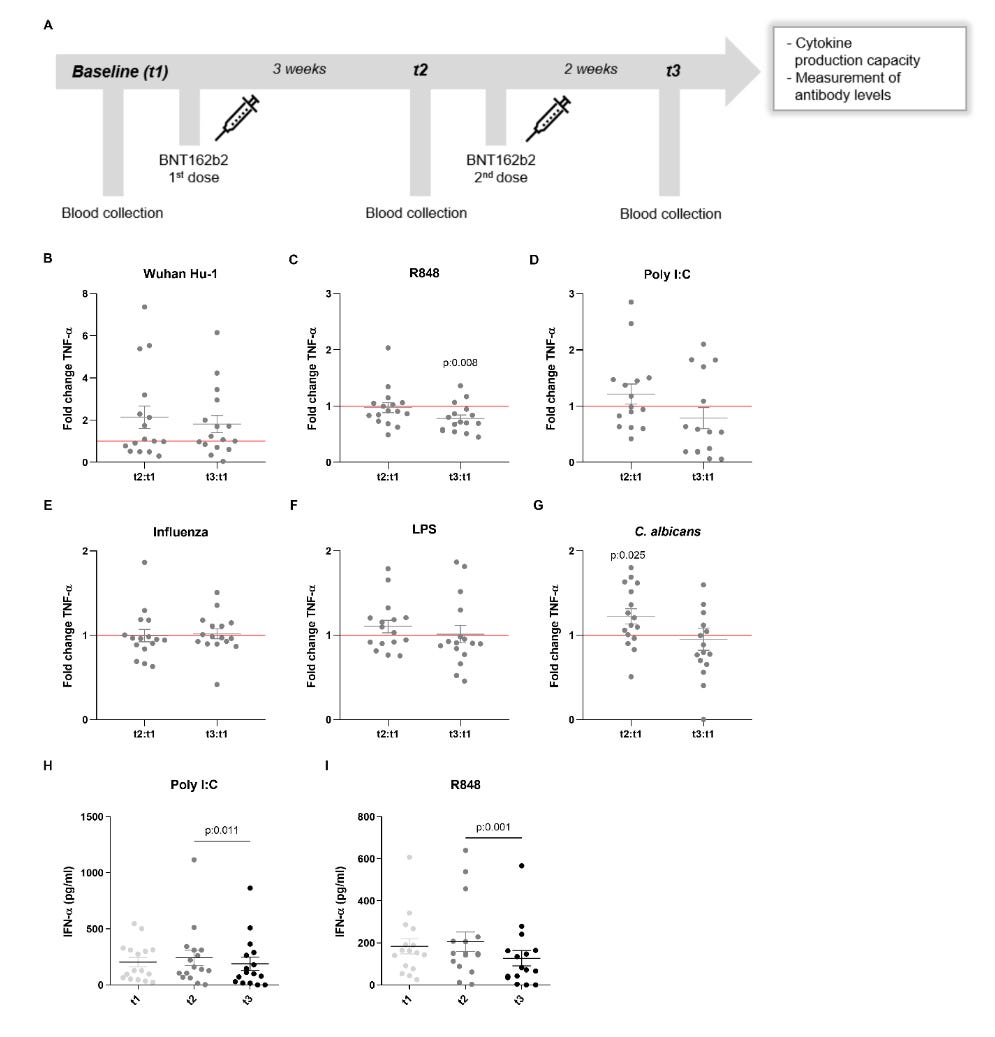
So dysregulated inflammation plays an important role in the pathogenesis and severity of COVID-19.9 There are studies that show that long-term innate immune responses can be either increased (trained immunity) or down-regulated (innate immune tolerance) after certain vaccines (such as Bacillus Calmette-Guérin (BCG) and the measles, mumps, and rubella (MMR) vaccines) or infections, so this is not a new thing.10 The way that the authors determined that the innate responses were being modulated in the context of the COVID-19 (the BNT162b2 one) injectables, was by checking out if the levels of certain measurable immune mediators produced in response to TLR stimulation using other virus, bacteria and fungi antigens, were ‘off’. Trained immunity (the one with decreases) is often measured by looking at the rustled-elevated-inflammatory cytokine (like monocyte-derived cytokines TNF-alpha, IL-1beta and IL-1Ra) leaves. When the TLR-3 and TLR-7 receptors were tickled, the amount of TNF-alpha production was way lower (significantly so for TLR-7) following dose 2 of the Pfizer stuff.
TNF-alpha production following stimulation with the TLR7/8 agonist R848 of peripheral blood mononuclear cells from volunteers was significantly decreased after the second [injection].
They also tickled the system with yeast (fungus) and found that the responses (specifically for IL-1beta - a fever-inducing interleukin) were higher following dose 1. The production of the anti-inflammatory cytokine IL-1Ralpha11 (the yin to the IL-1 yang) was reduced in response to a bacterial antigen (lipopolysaccharide (LPS)) and to yeast after the second injection - more evidence that there’s a shift to a stronger inflammatory response to fungal stimuli after injection. They also found that Interleukin-6 (IL-6) responses were similarly decreased, which is interesting, because IL-6 induces the liver to produce c-reactive protein which activates the complement system which helps antibodies out and promotes inflammation which means that doesn’t this mean that we should see less inflammation? So many questions. So very few answers.
Dysregulated continual synthesis of IL-6 plays a pathological effect on chronic inflammation and autoimmunity.12
You don’t say.
So that’s what they found in the paper, in a very small nutshell. Figure 3 shows the design and some of the results of their assays. It basically shows fold-changes in Interferon-gamma (IFN-gamma) (these guys activate macrophages and induce MHC-II molecule expression) and TNF-alpha in response to stimulation of blood cells from injected people using TLR stimulation with various pathogens.
The bottom line here is this. We know that innate responses are vital to a healthy and optimally-functioning immune system. They are vitally integrated with and into the adaptive responses as these two branches work in impeccable, complex harmony. We also know that there are cases where vaccines have caused dysregulation of innate responses in humans. We also know that something is very, very wrong with these COVID-19 injectable products with regards to persistent hyperinflammation and a plethora of systemic and physiologically-comprehensive adverse events including death from micro-emboli formation and clotting. We also know that these authors have now provided evidence to support that these COVID-19 injectable products are modulating innate responses and that this isn’t limited to problems with COVID-19. Problems with fungi, other viruses and bacteria can be anticipated. VAERS has hundreds of thousands of reports of adverse events related to fungal infections, plagues of herpes zoster occurrences (shingles) indicating weakened immunity, cancers coming out of remission, and the list goes on. And most of these reports are made for adults.
Here’s the thing…
Since children have extraordinary capabilities with regards to dealing with COVID-19 via their innate immune system responses, what will happen to them if these are not only by-passed by these injections, but knocked down by them?

Please listen to mighty baby. The kids are alright. Leave them alone. You might not get how this circles back the kids, but it does. Thanks for reading this to the end. And don’t inject kids with this stuff. You might mess them up and they don’t need it.
Nochi T, Kiyono H. Innate immunity in the mucosal immune system. Curr Pharm Des. 2006;12(32):4203-13. doi: 10.2174/138161206778743457. PMID: 17100623.
Rehwinkel J, Gack MU. RIG-I-like receptors: their regulation and roles in RNA sensing. Nat Rev Immunol. 2020 Sep;20(9):537-551. doi: 10.1038/s41577-020-0288-3. Epub 2020 Mar 13. PMID: 32203325; PMCID: PMC7094958.
Liu T, Zhang L, Joo D, Sun SC. NF-κB signaling in inflammation. Signal Transduct Target Ther. 2017;2:17023-. doi:10.1038/sigtrans.2017.23.
Bruce K. Patterson, Edgar B. Francisco, Ram Yogendra, Emily Long, Amruta Pise, Hallison Rodrigues, Eric Hall, Monica Herrara, Purvi Parikh, Jose Guevara-Coto, Xaiolan Chang, Jonah B Sacha, Rodrigo A Mora-Rodríguez, Javier Mora. Persistence of SARS CoV-2 S1 Protein in CD16+ Monocytes in Post-Acute Sequelae of COVID-19 (PASC) Up to 15 Months Post-Infection. bioRxiv 2021.06.25.449905; doi: https://doi.org/10.1101/2021.06.25.449905.
Xu H, Zhong L, Deng J, et al. High expression of ACE2 receptor of 2019-nCoV on the epithelial cells of oral mucosa. Int J Oral Sci. 2020;12(1):8. Published 2020 Feb 24. doi:10.1038/s41368-020-0074-x.
Fu J, Zhou B, Zhang L, Balaji KS, Wei C, Liu X, Chen H, Peng J, Fu J. Expressions and significances of the angiotensin-converting enzyme 2 gene, the receptor of SARS-CoV-2 for COVID-19. Mol Biol Rep. 2020 Jun;47(6):4383-4392. doi: 10.1007/s11033-020-05478-4. Epub 2020 May 14. PMID: 32410141; PMCID: PMC7224351.
National Center for Biotechnology Information (2021). PubChem Pathway Summary for Pathway WP4868, Source: WikiPathways. Retrieved December 16, 2021 from https://pubchem.ncbi.nlm.nih.gov/pathway/WikiPathways:WP4868.
Li SW, Wang CY, Jou YJ, et al. SARS Coronavirus Papain-Like Protease Inhibits the TLR7 Signaling Pathway through Removing Lys63-Linked Polyubiquitination of TRAF3 and TRAF6. Int J Mol Sci. 2016;17(5):678. Published 2016 May 5. doi:10.3390/ijms17050678.
Tahaghoghi-Hajghorbani S, Zafari P, Masoumi E, Rajabinejad M, Jafari-Shakib R, Hasani B, Rafiei A. The role of dysregulated immune responses in COVID-19 pathogenesis. Virus Res. 2020 Dec;290:198197. doi: 10.1016/j.virusres.2020.198197. Epub 2020 Oct 16. PMID: 33069815; PMCID: PMC7561578.
Alberto Mantovani, M.D., and Mihai G. Netea, M.D.. Trained Innate Immunity, Epigenetics, and Covid-19. NEJM 383;11 nejm.org September 10, 20201078.
Arend WP. Interleukin-1 receptor antagonist. Adv Immunol. 1993;54:167-227. doi: 10.1016/s0065-2776(08)60535-0. PMID: 8379462.
Tanaka T, Narazaki M, Kishimoto T. IL-6 in inflammation, immunity, and disease. Cold Spring Harb Perspect Biol. 2014;6(10):a016295. Published 2014 Sep 4. doi:10.1101/cshperspect.a016295.
No comments:
Post a Comment